Effective Treatments for Alcholism
If you have tried to stop drinking and found yourself back in the same pattern days or weeks later, you already know this problem is not about weak willpower. How alcohol addiction is treated depends on the severity of drinking, the presence of withdrawal symptoms, relapse history, mental health stress, and whether standard approaches have already failed. Effective treatment starts by identifying what is keeping the drinking cycle in place and then intervening with a plan strong enough to break it.
For some people, alcohol use has become woven into stress relief, sleep, social habits, and emotional avoidance all at once. For others, the pressure is more immediate—family conflict, job risk, legal trouble, or a required alcohol evaluation. In either case, waiting for the problem to “settle down” rarely works. Treatment works better when it is direct, individualized, and designed around the real reasons a person keeps drinking.
How alcohol addiction is treated in real clinical practice
Treatment is not one single event. It is a sequence. First, a clinician has to determine whether a person can stop safely and what level of support is needed. Then the work shifts toward reducing cravings, interrupting habits, and building enough structure that alcohol is no longer running the day.
That is why responsible treatment usually begins with assessment. A provider looks at how much and how often a person drinks, whether morning drinking is happening, whether blackouts have occurred, whether withdrawal symptoms show up when alcohol is reduced, and how many failed quit attempts have already happened. Family pressure, work consequences, court involvement, and physical health symptoms also matter. Two people can both say, “I drink too much,” while needing very different levels of care.
For one person, treatment may begin with medically supervised detox. For another, the right starting point may be outpatient counseling, hypnosis, acupuncture, behavioral support, or a deterrent-based approach meant to make drinking physically undesirable. The right plan is not the most familiar one. It is the one that addresses the actual pattern.
The first stage: stopping safely
One of the biggest mistakes people make is assuming they can simply quit cold turkey without consequences. Alcohol withdrawal can range from anxiety, shaking, sweating, nausea, and insomnia to severe medical complications. If someone has been drinking heavily or daily, their safety must be the top priority.
This is where professional screening matters. A proper evaluation can identify whether withdrawal risk is mild, moderate, or dangerous. If detox support is needed, that stage should happen before deeper behavioral treatment begins. Trying to work on relapse prevention while the body is still in acute withdrawal is rarely effective.
Even when withdrawal is not medically severe, the early phase of stopping alcohol is physically and emotionally disruptive. Sleep is off. Irritability spikes. Cravings come in waves. The person may feel restless, exposed, or mentally scattered. Effective treatment prepares for that reality instead of pretending motivation alone will carry the process.
What actually changes drinking behavior
Once the person is stable enough to engage in treatment, the next goal is changing the pattern that keeps alcohol in control. That usually means working on both the psychological pull of drinking and the ritual of it.
Many people drink for reasons they can name only partly. Stress is one answer, but not the whole answer. Alcohol may also be tied to reward, emotional numbing, loneliness, social confidence, anger management, boredom, grief, or self-punishment. A treatment approach that ignores those drivers may produce short-term compliance but weak long-term change.
Behavioral treatment helps a person identify triggers, anticipate high-risk moments, and replace automatic drinking responses with more deliberate action. That sounds simple when written out, but in practice it takes repetition and accountability. The old pattern is quick, familiar, and reinforced. The new pattern has to be practiced enough to become usable under pressure.
This phase is also where personalized care matters. Some people need direct intervention and firm structure. Others respond better when treatment reduces internal resistance and addresses subconscious habits. If a person has already gone through conventional methods without lasting success, a different therapeutic path may be the more practical one.
Why alternative methods can help when standard approaches have not
Are alternative methods the best answer to how alcohol addiction is treated? A major reason people delay treatment is that they assume their only option is a traditional rehab model that does not fit their life, preferences, or prior experience. That is not always the case. Alternative and holistic services can play a meaningful role in alcohol treatment when people use them purposefully and as part of a focused plan.
Hypnosis and hypnotherapy, for example, can help interrupt entrenched mental associations around alcohol. For some patients, drinking becomes so tightly linked to relaxation, relief, or 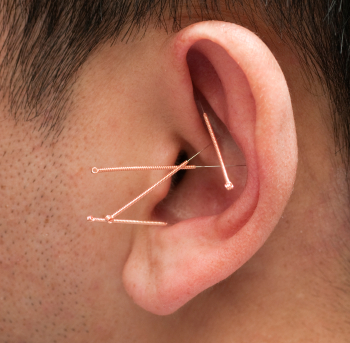 escape that conscious reasoning alone cannot change the behavior. Hypnotic work can directly address cravings, anticipatory thinking, self-sabotage, and conditioned triggers in a way that talk alone cannot.
escape that conscious reasoning alone cannot change the behavior. Hypnotic work can directly address cravings, anticipatory thinking, self-sabotage, and conditioned triggers in a way that talk alone cannot.
Auricular acupuncture using the NADA protocol is another option that many patients consider useful during early recovery and high-stress periods. It is not a magic fix, and it is not meant to replace proper assessment or clinical treatment. What it can do is support regulation—easing agitation, reducing tension, and helping the nervous system settle enough for treatment to take hold. For someone who feels constantly activated when trying to stop drinking, that can make a real difference.
Some patients also benefit from alcohol deterrent treatment designed to create a strong physical and psychological barrier to relapse. This kind of intervention is not right for everyone, but for the right person it adds consequence where impulse has repeatedly won. When relapse has become too automatic, increasing the cost of drinking can be a powerful clinical tool.

At Philadelphia Addiction Center, this kind of nontraditional care is not treated as an add-on or a novelty. It is used as part of a serious treatment strategy for people who need a more targeted intervention than standard advice has provided.
Psychological Coding for Alcoholism
One of the most successful therapies used by narcologists in the United States and around the world for alcoholism is psychological coding. And that’s how alcohol addiction is treated in alternative medicine clinics. Can hypnosis help me give up alcohol? Everyone is aware that alcoholism is a sickness by this point. Although there is no cure for alcoholism, it can be prevented. An alcoholic must give up drinking entirely to lead a normal life. A person who becomes unwell will always be an alcoholic; they will never be able to drink in moderation or in tiny doses. He or she must decide whether to completely and permanently give up drinking or perish. Sober alcoholics or abstinent drinkers are those who decide to live. “An  alcoholic cannot become a moderate drinker, just as it’s impossible to turn a pickled cucumber into a fresh one” is a common joke among sober drinkers.
alcoholic cannot become a moderate drinker, just as it’s impossible to turn a pickled cucumber into a fresh one” is a common joke among sober drinkers.
The practice of using different psychotherapy techniques and the patient’s mental resources is known as psychological coding for alcoholism, or psychotherapeutic coding for alcoholism. This approach is stable and long-term. One of the earliest and most reliable methods for treating alcoholism is psychological coding. Before the early 20th century, when researchers created anti-alcohol medications and antidepressants, psychoanalytic treatment for alcoholism and autogenic training were already in use. Patients improved steadily and were able to permanently give up alcohol thanks to the treatment. Alcohol therapy with psychology is dependable and safe. Nevertheless, it takes a long time because the cancerous signs that have been there for years cannot be removed in a matter of minutes or hours. A patient’s willingness and patience are insufficient to use their mental reserves, as they also need a reasonable length of time. One of the requirements for a successful course of treatment is collaboration between the patient and the physician. The most popular treatment for alcoholism combines behavioral and psychoanalytic therapy, neuro-linguistic programming, and hypnosuggestive therapy. This method works well for patients who want to comprehend their errors and misunderstandings and alter their behavior. This method of treatment is especially recommended for people who become dependent on alcohol due to prolonged heavy drinking.
Disulfiram Implant Esperal for Alcoholism
The most recent and efficient kind of disulfiram implant was created by the French company ESPERAL. The apparatus is a thin-film microchip with a dispenser that holds five dry, 100% concentrated disulfiram crystals. Every fifteen minutes, the bio-circuit ESPERAL measures the amount of alcohol in the patient’s blood; if it exceeds 0.05, one crystal of disulfiram is dropped into the surrounding capillaries. The disulfiram-ethanol response starts in around 35 to 50 seconds and is painless. The immune system’s reaction is really harsh. Once the disulfiram-ethanol combination starts, it cannot be stopped, and the 911 team has no control over it. It lasts five to eight hours, depending on body weight, and only ends when the disulfiram crystal finally runs out. Therefore, the Philadelphia Hypnotherapy Clinic offers disulfiram implants if you want to take advantage of their impressive results. To assist you in managing your condition, Dr. Tsan will provide expert assistance. It is the most cutting-edge strategy for combating alcoholism. Additionally, studies have demonstrated that it improves the effectiveness of alcoholism treatment.
How treatment is adjusted for different situations
No honest provider should claim there is one best method for everybody. It depends on the pattern, the urgency, and the obstacles.
A person drinking every day with withdrawal symptoms needs a different starting point than someone who binge drinks heavily on weekends but can abstain during the week. Someone facing court requirements may need formal documentation, structured compliance, and clear treatment milestones. Someone else may be more concerned with privacy, discretion, and stopping quickly before family or work consequences escalate.
Relapse history also changes the plan. If a person has already tried counseling, support meetings, or self-directed abstinence and still returned to drinking, treatment should not simply repeat the same formula with different wording. It should become more precise. That may mean adding hypnotic work, more frequent therapeutic contact, acupuncture support, a deterrent intervention, or closer monitoring during high-risk periods.
Mental and emotional strain matter too. Some people drink to shut off anxiety at night. Others drink after conflict, shame, or frustration. If treatment does not address those moments, the person may stay sober temporarily while remaining highly vulnerable. Real treatment identifies the pressure points before they become the next relapse.
The role of accountability and follow-through
Secrecy and delay often sustain alcohol addiction. People promise themselves they will stop Monday, after the holiday, after the court date, after one more stressful week. Meanwhile, the drinking pattern becomes stronger. Good treatment interrupts that cycle by creating structure now, not someday.
Accountability does not have to mean punishment. It means that treatment is active, measurable, and difficult to avoid. Appointments are kept. progress is reviewed. Relapse risks are addressed early. If a method is not working, the plan changes instead of drifting.
This is especially important for those who say, “I know what I should do; I just don’t do it.” Knowledge is not the missing ingredient in most alcohol problems. Intervention is. The right treatment creates enough external support and internal change that action finally starts matching intent.
What people should expect from effective alcohol treatment
People often ask how alcohol addiction is treated and how long treatment takes. The honest answer is that the timeline varies, but early improvement should not feel vague. Within the first phase of effective care, a person should have more clarity about their triggers, a safer strategy for stopping, and a treatment path that feels specific to them rather than generic.
That does not mean every day is easy. Cravings can still show up. Ambivalence can still show up. Some people feel better quickly, but then they may struggle again as the initial excitement fades. That is normal. What matters is whether the treatment plan is built to handle those turns.
A strong program should help the person regain control, reduce the compulsive pull of alcohol, and strengthen the ability to function without relying on drinking as the answer to every difficult feeling. It should also respect the fact that many people want effective help without disappearing into a one-size-fits-all rehab system.
If alcohol has started deciding too much of your life, the next step should be more than advice. It should be a real intervention, matched to your pattern, your risk level, and your goals, because change becomes much more possible once treatment stops being generic and starts being personal.
How Alcohol Addiction is Treated at the Philadelphia Addiction Center—the #1 Outpatient Treatment Facility for Alcohol Abuse
So, now that you know how alcohol addiction is treated, find the best place for your program. While alcoholism treatment centers are located in almost every state of the US, not all of them can prove a high success rate in the treatment of alcohol abuse. Philadelphia Addiction Center, the subdivision of the Philadelphia Holistic Clinic, is known as the home for the “Esperal Implant” on the East coast of the USA. The success rate of the treatment provided at the center is way above average in the industry.
For more information about Esperal treatment for alcohol abuse, contact Philadelphia Addiction Center at (267) 403-3085